

{kind=link}
Renewing ACLS Online? Learn the most common mistakes healthcare professionals make and how to choose a course that supports patient care.

As practitioners of ACLS, it is important to develop an understanding of several conditions that can affect the heart. This understanding combined with critical thinking skills will allow you to treat root causes of non-homeostasis, including hyperkalemia.
A popular mnemonic used as a prompt during ACLS training is to “consider the H’s and T’s” – otherwise known as the reversible causes of pulseless arrest including PEA, asystole, ventricular fibrillation, and ventricular tachycardia. As a quick reminder, the H and T pneumonic includes the following:
Figure 1: “H’s and T’s”
| H’s | T’s |
|---|---|
| Hypovolemia | Toxins |
| Hypoxia | Tamponade (cardiac) |
| Hydrogen ion acidosis | Tension pneumothorax |
| Hyper (or hypo) kalemia | Thrombosis (coronary or pulmonary) |
| Hypoglycemia | Trauma |
| Hypothermia |
The focus of this study is on hyperkalemia, which is defined as a serum potassium concentration that is too high. It is officially considered high if it is greater than the normal range of 3.5-5.3 mEq/l. Let’s look further into the causes, symptoms, and treatments used for hyperkalemia, specifically in an ACLS situation.
Potassium is one of the most important electrolytes in the human body. It works in tandem with other electrolytes, including chloride, calcium, phosphorus, magnesium, and sodium. Potassium has important roles in the functioning of all of the body’s cells, tissues, and organs. It performs critical roles in nerve conduction, controlling the amount of water in the body, and maintaining a healthy blood pH level.
Potassium is the most abundant ion in the intracellular fluid. Potassium’s positively charged ions work opposite of sodium’s negatively charged ions. Potassium is also alkaline in nature and helps to balance acidic environments. Its movement in and out of the cell to maintain a stable serum potassium level (KCl) is controlled by the action of the body’s sodium-potassium pump (ATPase), found in the cell membranes. The NaK pump moves potassium ions into the cell, while at the same time moving sodium ions out of the cell.
The sodium-potassium pump is used throughout the body, for many different functions:
Although potassium effects processes all over the body, our focus will be on cardiac effects that induce lethal heart rhythms. As part of the ACLS algorithm, correcting underlying potassium imbalances quickly can be the key to a successful cardiac resuscitation.
Most cases of mild hyperkalemia are tolerated well without many symptoms. Most of the time, the body is able to self-correct the condition. However, when mild hyperkalemia progresses into severe hyperkalemia, it can result in dangerous effects, such as cardiac arrest. Extremely high levels of serum potassium are associated with a high mortality rate. Severe hyperkalemia is generally associated with levels over 7.0 mEq/L, although symptoms may be present at levels over 6.0mEq/L.
Figure 2: Normal and Elevated Potassium Levels
| Condition | Serum Potassium Level |
|---|---|
| Normal | 3.5 – 5.0 mEq/L |
| Mild Hyperkalemia | 5.1 – 6.0 mEq/L |
| Moderate Hyperkalemia | 6.1 – 7.0 mEq/L |
| Severe Hyperkalemia | >7 mEq/L |
Hyperkalemia is very rarely caused by consuming too much dietary potassium. The cause is typically an underlying condition in the body that interferes with the exchange or excretion of potassium ions.
The major causes of hyperkalemia are:
The kidneys normally excrete extra potassium through the urine to take care of any extra buildup in the body. Conditions that reduce the kidney’s ability to excrete electrolytes properly can result in hyperkalemia. These include both acute and chronic renal failure, glomerulonephritis, lupus nephritis, transplant rejection, and obstructions of the urinary tract (such as kidney stones).
Patients with kidney disease are also very susceptible to effects from using certain medications that can increase blood potassium levels. They will not excrete them as rapidly, and levels can build up in the blood.
Located beside the kidneys, the adrenal glands secrete cortisol and aldosterone, which perform important functions in homeostasis. Aldosterone prompts the kidneys to retain sodium and fluids, and to excrete potassium. Because of this important action, adrenal diseases such as Addison’s disease can cause hyperkalemia due to a decrease in aldosterone secretion. The body then retains potassium and suffers the effects of hyperkalemia.
Serum potassium measures the amount circulating in the blood at any given time. However approximately 98% of the potassium in the body is stored within the cells (intracellular). This explains how patients can have sudden increases in potassium levels, even though the total measurement of potassium in the body has not changed.
There are several conditions that can cause potassium to shift from the intracellular space to the extracellular space (the bloodstream). One of the most common is diabetic ketoacidosis (DKA). This condition most often occurs in Type I diabetic patients when they have too high of a concentration of glucose in their blood. The body breaks down fat stores for energy, causing a release of acidic ketones in the blood. This causes fluids and potassium to move out of the cells into the blood circulation in an attempt to thin the blood and normalize pH — thus resulting in hyperkalemia. Additionally, many diabetic patients have reduced kidney function, which causes difficulty excreting this extra potassium.
Another overall reason for potassium shift is tissue destruction – which can occur in many ways. As cells are destroyed in the body, they release their contents into the bloodstream, including stored potassium. Tissue destruction occurs with:
In an ACLS scenario, it is important to obtain information about the patient’s medical history and medication usage. Hyperkalemia, especially in the presence of kidney dysfunction, can be caused by several types of medication.
Medications can interfere with potassium homeostasis by several different mechanisms of action:
Figure 3: Common Drugs that can cause Hyperkalemia
| Drugs Class/Action | Common Names | Mechanism of Action |
|---|---|---|
| ACE inhibitor - antihypertensive | Ramipril, Lisinopril, Altace. *Medication names commonly end in -pril. | Disrupts the renin-angiotensin-aldosterone cycle by inhibiting angiotensin converting enzyme (ACE). This prevents Angiotensin I from converting to Angiotensin II. |
| Angiotensin II receptor blockers (ARBS) - antihypertensive | Diovan (valsartan), Micardis (telmisartan), Avapro (irbesartan) *Medication names commonly end in -sartan. |
Disrupts the renin-angiotensin-aldosterone cycle by preventing Angiotensin II from binding to Angiotensin II receptors. |
| Potassium-sparing diuretics – antihypertensive, diuretic | spironolactone (Aldactone); eplerenone, (Inspra); amiloride (Midamore) | Interferes with potassium/sodium exchange in the distal convoluted tubule of the kidneys and blocks aldosterone receptors. |
| Calcium-channel blockers - antiarrhythmic | Verapamil, nifedipine, diltiazem | Interferes with potassium/sodium exchange in the kidney by blocking aldosterone production. |
| NSAIDs - analgesic | Ketorolac (Toradol); diclofenac (Voltaren); naproxen (Aleve); ibuprofen (Motrin, Advil); meloxicam (Mobic) | Inhibits COX-2 isoforms present in the kidney. This reduces renal prostaglandins that promote renin and aldosterone excretion. Also partially blocks antidiuretic hormone. |
| Heparin - anticoagulant | Both low molecular weight and unfractionated heparin preparations. | Blocks a step in the synthesis of aldosterone, causing hypoaldosteronism, resulting in hyperkalemia. |
Most people do not display noticeable symptoms until their potassium reaches the level of around 7.0 mEq/L, especially if the level has risen slowly, or they suffer from chronic kidney disease.
Too much potassium outside of the cell changes the gradient, and the way in which the sodium-potassium ATPase pump generates a nerve impulse. This extra potassium causes a slowdown in the process, resulting in delayed nerve impulses – or in some cases none at all. This results in decreased reflexes, tingling, and numbness.
Nerves typically fulfill their role of stimulating cardiac, skeletal, and smooth muscle fibers to contract. When the nerves are not functioning properly, neither do the muscles. This causes symptoms like muscle weakness and, in rare cases, paralysis.
The smooth muscle that makes up the GI tract is also affected by hyperkalemia. It stretches from the esophagus to the colon. Peristalsis becomes weak as a result of hyperkalemia, which can result in gas and bloating, nausea, vomiting, and diarrhea.
Heart cells, called myocytes, also depend on nerve conduction to receive the signals to keep the heart beating. When hyperkalemia occurs, contractions of the heart become less forceful, the heart rate slows down, and sometimes abnormal heart rhythms develop. This situation can be life-threatening and result in cardiac arrest.
One of the most readily accessible tools to find underlying hyperkalemia is the ECG. Certain ECG changes are characteristics of hyperkalemia, although these do not always occur in every case. Note that hyperkalemia does not always cause ECG changes, and conversely sometimes ECG changes are seen in serum potassium levels below 7.0 mEq/L.
The first (and most common) change is a “tall T” or increase in amplitude of the T wave. This is especially helpful when it can be compared to a previous ECG. This typically occurs with moderate hyperkalemia and indicates repolarization abnormalities.
Figure 4: Hyperkalemia and tall T-waves
.png)
Source: https://www.ekgrhythm.com/2015/11/tall-t-waves-due-to-hyperkalemia.html
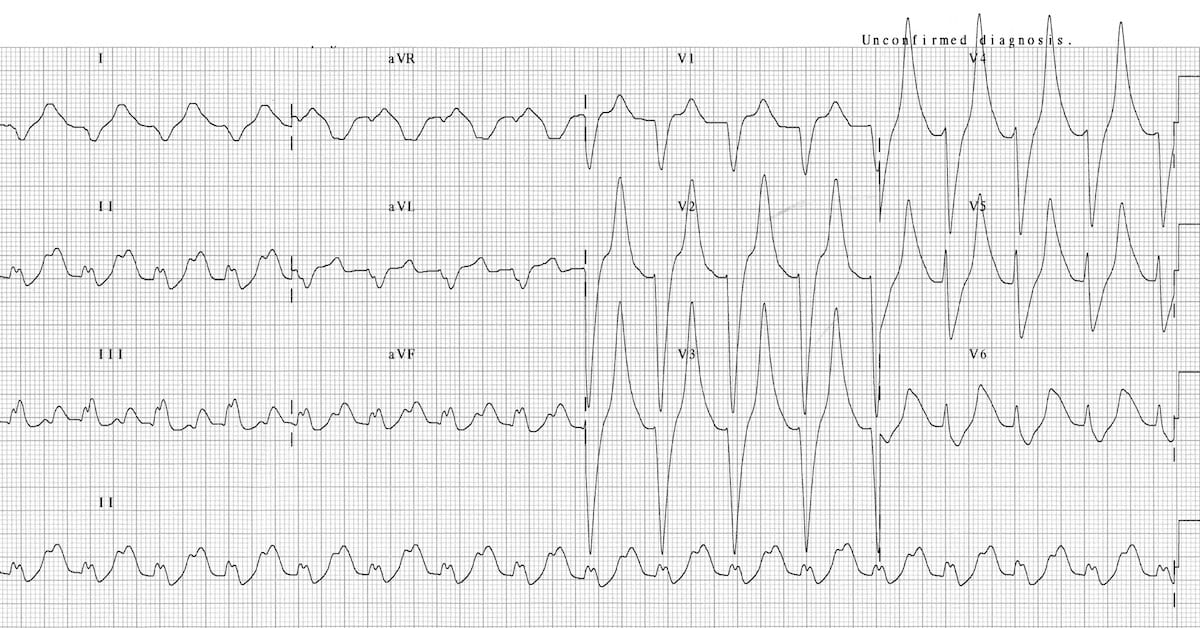
As hyperkalemia progresses, other conduction problems may be displayed on the ECG, like flattening of the P-wave, a prolonged PR interval, and widening of the QRS complex (along with the tall T wave).
Figure 5: ECG with prolonged QRS peaked T-waves, flattened P-wave.

Source: https://litfl.com/wp-content/uploads/2018/08/ECG-Hyperkalemia-serum-potassium-9.3.jpg
After the appearance of wide, bizarre QRS complexes with obvious conduction blocks, the ECG can then degrade into lethal rhythms like asystole, ventricular fibrillation (VF) or pulseless electrical activity (PEA).
With all of the background knowledge above, you can identify clues that can indicate hyperkalemia even when the patient is unconscious. The presence of ECG changes indicative of hyperkalemia, with some additional knowledge about the patient’s history, medications, and comorbid conditions, can lead the ACLS team to try to reverse probable hyperkalemia. Hyperkalemia in hospitalized patients is more likely caused by a combination of factors, such as hypovolemia, renal dysfunction, plus an ACE inhibitor medication. Successful treatment may mean addressing several of these factors at the same time.
Once hyperkalemia is suspected or confirmed, there are several methods of treatment that can be used. The method selected depends on the condition of the patient and the suspected cause of the hyperkalemia.
In an ACLS situation, the goal is to stabilize the potassium level and the patient as quickly as possible. This means that slower, gentler means of lowering the potassium level are excluded.
IV calcium gluconate or chloride is indicated in the presence of ECG changes or a potassium level greater than 6.5 mEq/L.
Figure 6: Calcium dosing
| Peripheral IV Access | Central V Access | |
|---|---|---|
| Initial Dosage | 3 Grams IV calcium gluconate over 10 minutes | 1 Gram IV calcium chloride over 10 minutes or slow IV push. |
| Subsequent Dosage | **May be indicated for persistent arrhythmias. However, point-of-care electrolyte testing should ideally guide dosing. Calcium lasts for about 30-60 minutes, so treatment may need to be repeated for this reason. | **May be indicated for persistent arrhythmias. However, point-of-care electrolyte testing should ideally guide dosing. Calcium lasts for about 30-60 minutes, so treatment may need to be repeated for this reason. |
The combination of IV dextrose and IV insulin is used to shift serum potassium back into the cells. A baseline fingerstick glucose level should be taken, then the glucose level monitored frequently for four to six hours after this infusion.
The resulting potassium shift should last for several hours but may need to be re-dosed or accompanied by another treatment.
While administering beta-2 agonists don’t cause as large a shift of potassium back into the cells as other treatments do, they do cause a small shift. Typically, these methods are used as a combination treatment or if a specific cause of the hyperkalemia is known. Another specific scenario might be in the case of no IV access.
Isotonic (not hypertonic) bicarbonate solution, given IV, is recommended in the case of known metabolic acidosis. Bicarbonate decreases the serum potassium via three methods:
This treatment requires giving at least 1-2 liters of fluids, so it is not recommended for patients in fluid overload or renal failure.
In the absence of kidney failure (chronic or acute), kaliuresis can be used to remove excess potassium from the body. This is accomplished by administering IV loop diuretics, such as furosemide (Lasix) or bumetanide (Bumex), combined with a thiazide diuretic such as hydrochlorothiazide (HCTZ) and Acetazolamide. Electrolytes should be monitored, as well as the patient’s kidney function and fluid intake and output. In the process of removing excess potassium, the patent may become hypovolemic. Fluid resuscitation may be necessary.
In the case of renal impairment or failure, emergent hemodialysis will be necessary to excrete excess potassium from the body.
Sodium Polystyrene Sulfonate (brand names Kayexalate, Kionex, and Kalexate) are not used for emergent treatment of hyperkalemia, because they work slowly. However, they may be used afterward as ongoing treatment.
These medications are given orally and work by binding with potassium in the digestive tract. It typically causes the patient to excrete excess potassium through the feces, and may cause diarrhea, nausea, and lack of appetite.
Hyperkalemia is a condition that can disrupt homeostasis in several ways, thus causing critical cardiac conditions. Because of its many causes, hyperkalemia is a condition that is frequently seen in hospitalized patients. It is likely that ACLS-trained clinicians will encounter hyperkalemia in the context of an ACLS response and should understand the likely causes and emergent treatment of this condition.
To learn more about the clinical scenarios, drugs, ECG rhythms, and other topics related to ACLS, high-quality study materials are available through AMRI. Accredited by the National Board of Emergency Care Certifications (NBECC), AMRI has helped more than one million medical professionals earn their ACLS, BLS, and PALS certifications or recertifications since 1983.
Register for your exam with AMRI today to gain access to premium study materials and our widely accepted certification program.